Do Endometrial Polyps Impact My Fertility?
If you are reading this, chances are you have just been told that you have a uterine (endometrial) polyp, and your mind is racing with questions: Is this the reason I am not getting pregnant? Do I need surgery? What if this changes everything? If you are feeling anxious, overwhelmed, or even a bit lost, you are not alone. Many women and couples in your shoes have faced the same worries. The truth is, endometrial polyps are a grey zone of fertility medicine: much talked about, often misunderstood, and surrounded by conflicting opinions. Let’s break this down together—no jargon, no sugarcoating, just clear facts and real hope.
What Are Endometrial Polyps and Why Do They Happen?
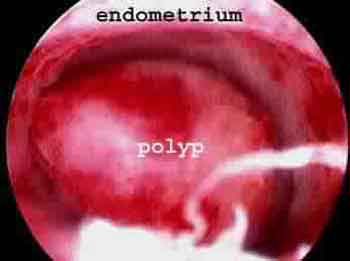
Endometrial polyps are soft, fingerlike growths that develop in the lining of the uterus (the endometrium). Think of them as small bumps or skin tags inside the womb, caused by an overgrowth of the cells that line the uterus. They are hormonally driven, meaning they tend to grow when estrogen levels are high (usually in the first half of your cycle).
Most women with polyps will never know they have them. They are usually silent, causing no pain or symptoms at all. Occasionally, some women may notice:
- Irregular or heavy periods
- Spotting between cycles
- Bleeding after intercourse
- Difficulties with conception that seem unexplained
But for many, these polyps are discovered incidentally during fertility tests or scans. And when that happens, it is natural to wonder if this is the missing piece to your fertility puzzle.
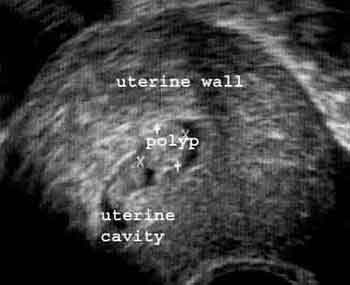 Fig 2. Uterine polyp seen during ultrasound scan after infusion of saline which outlines the polyp in the cavity
Fig 2. Uterine polyp seen during ultrasound scan after infusion of saline which outlines the polyp in the cavity
How Are Polyps Detected? Timing Makes All the Difference
Detecting a uterine polyp is a bit like trying to spot a snowflake in a blizzard—the timing and method matter a lot. Polyps are easiest to see when the lining of your uterus is thickest, which happens around Day 10 to 12 of your menstrual cycle (when estrogen peaks). If your ultrasound is done at a different time, your doctor might miss it entirely.
- Transvaginal Ultrasound: A standard scan may spot larger polyps, but small ones can be missed unless the test is precisely timed.
- Saline Infusion Sonography (Sono-HSG): This test involves gently filling the uterus with saline during the scan, making polyps stand out more clearly against the fluid. It’s a simple, clinic-based procedure that significantly improves accuracy.
- Hysteroscopy: This is the gold standard. A tiny camera is passed through the cervix to look directly inside the uterus. Not only does this confirm the presence of a polyp, but it also allows for immediate removal if needed. You can read more about the procedure here.
Even with perfect scans, small polyps can be missed if the test is not done at the right phase of your cycle.
Sometimes, a hysterosalpingogram (HSG) may pick up a polyp as a 'filling defect' inside the uterus, but this test is not as reliable for polyps as the others mentioned above.
Do Polyps Really Affect Fertility? What the Science (and Experience) Says
Here is where things get tricky. Doctors and clinics all over the world debate whether small polyps actually cause infertility or failed IVF cycles. Some polyps might block the ‘pathway’ for sperm to meet the egg, interfere with implantation, or trigger mild inflammation that makes it harder for an embryo to settle in. Yet, plenty of women with polyps get pregnant naturally and never know they had one at all.
On the other hand, studies have shown that removing polyps can improve pregnancy rates in some women struggling with unexplained infertility—especially if the polyp is located near the opening of the fallopian tube (where eggs enter the uterus), or if there are several polyps present.
Pregnancy rates reported after polyp removal in women with unexplained infertility, according to research studies. Results can vary, but the numbers offer hope for many.
For couples considering IVF, most fertility specialists recommend removing any polyps detected before embryo transfer. The reasoning is simple: if there is anything inside the uterus that could even potentially hinder implantation, it is better to clear it out first. Still, some doctors argue that very small polyps (less than 1 cm) may be harmless, and removing them could be unnecessary.
Medical science does not always have black-and-white answers. Sometimes, the best decision is based on your unique story, not just statistics.
Should All Polyps Be Removed? The Honest, No-Nonsense Answer
This is the real dilemma. There is no universal right answer because every patient, every polyp, and every fertility journey is different. Here’s what you need to know to make the best decision for yourself:
- Size matters, but location matters more. Polyps near the opening of the tube or those sticking out into the cavity may create more problems than tiny ones flat against the wall.
- Symptoms count. If you have abnormal bleeding or pain, removal is usually advised.
- Fertility plans matter. If you are about to begin IVF, most experts recommend clearing the uterine cavity of any polyps to maximize your chances.
- Some polyps go away on their own. About a quarter of small polyps may shrink or vanish, especially in younger women.
- There are risks to surgery, but modern techniques are safe. Hysteroscopic removal is a minor procedure, often done as day care, with minimal recovery time.
At Malpani Infertility Clinic, we believe you deserve a tailored, evidence-based approach—not just standard recipes. We discuss the risks and benefits openly, and together, decide what is right for your unique circumstances. We want you to be in control of your health decisions, armed with real information (not just opinions or pressure).
What Happens If You Decide to Remove the Polyp?
If you and your doctor choose to remove the polyp, the procedure is usually straightforward. Using a hysteroscope (a slim, lighted camera), the doctor can see inside your uterus and remove the polyp precisely, minimizing disturbance to the healthy lining. Recovery is quick—most women go home the same day and can resume normal activities within 24-48 hours.
Older approaches like D&C (dilation and curettage) are less commonly used now because they are less precise and can sometimes miss the polyp or cause more trauma to the uterine lining. Hysteroscopic removal is safer, more accurate, and gives us a chance to confirm that the polyp is entirely gone.
Some women notice improved cycles or even spontaneous pregnancies after polyp removal. For others, it clears the way for a successful IUI or IVF cycle. Either way, you have taken an informed step forward—one that is backed by both science and experience.
Frequently Asked Questions
Q: Can a small endometrial polyp really prevent me from getting pregnant?
A: Most small polyps do not cause infertility, but in some cases—especially if they are near the tube opening or cause inflammation—they might interfere with implantation or sperm movement. Discuss your individual risks with your doctor.
Q: Is it absolutely necessary to remove a polyp before IVF?
A: There is no strict rule, but many experts recommend removing polyps before embryo transfer to optimize the uterine environment. Decisions should be personalized based on size, location, and your fertility history.
Q: Will the removal procedure hurt? What is the recovery like?
A: Hysteroscopic polyp removal is minimally invasive and typically done as a day procedure. Most women feel mild cramps for a short time and return to normal activities within a day or two.
Q: How do I know if my polyp will go away on its own?
A: Some small polyps can disappear naturally, especially in younger women. The decision to wait or remove depends on your symptoms, fertility plans, and doctor’s advice.
Q: Are there any risks with leaving a polyp untreated?
A: Most polyps are benign and cause no harm. However, rarely, they can grow or cause bleeding, and some (especially larger or persistent ones) could affect fertility or mask other conditions. Regular follow-up helps ensure peace of mind.