The Fallopian Tubes and Tubal Infertility

Every month, so many hopeful couples sit across from a fertility specialist and ask: Why am I not getting pregnant when everything seems normal? If you have ever wondered whether your fallopian tubes might be the missing piece, you are not alone. Tubal infertility is one of the most misunderstood and frustrating roadblocks on the path to parenthood, especially because its symptoms are often invisible and its diagnosis can feel overwhelming. This article is for those who want honest answers, clear explanations, and a sense that someone truly understands the fear and confusion of “unexplained infertility.”
What are the Fallopian Tubes and Why Do They Matter?
Most people never think about their fallopian tubes until they are told there might be a problem. These slender, flexible tubes project from each side of the uterus, acting as the crucial bridge between your ovaries and your womb. Measuring about 10 centimeters, the tubes end in delicate, finger-like fringes called fimbriae. When you ovulate, the fimbriae sweep the egg into the tube, starting the journey towards possible fertilization.
The fallopian tube is not just a simple pipe. It is a living, dynamic organ. Its muscular walls contract in a coordinated way to move the egg, and its lining is covered with microscopic cilia (tiny hair-like structures) that help push both the egg and—if things go well—the embryo along. The tube also produces nourishing fluid, supporting fertilization and early embryonic development.
Fertilization usually happens in the outer part of the tube (the ampulla). After the sperm meets the egg, the embryo travels down toward the uterus, arriving just at the right time for implantation, about four to seven days after ovulation. If the tubes are not working, this beautiful, complex process gets interrupted.
Fig 1. Normal tube and ovary, as seen during laparoscopy
How Do Tubal Diseases Cause Infertility?
Tubal factor infertility is far more common than most people realize. It is responsible for up to half of all cases of female infertility. The most usual culprit is damage to the tubes from infection or inflammation. What makes this so difficult for many women: you may never have had any obvious symptoms, or you might not even remember a significant illness.
- Sexually transmitted infections (like Gonorrhea or Chlamydia)
- Infections after childbirth, miscarriage, abortion, or after inserting an intrauterine device (IUD)
- Complications after abdominal or pelvic surgery (for example, removal of an ovarian cyst or a burst appendix)
- Severe endometriosis (a condition where tissue similar to the lining of the womb grows outside it)
- Tuberculosis (especially common in some parts of India, often spreading silently from the lungs to the reproductive organs)
All these issues can cause the tubes to become blocked or stick to other organs. Scar tissue (called adhesions) may develop, making it even more difficult for the egg and sperm to meet. What is especially unfair: many women with tubal damage have never felt sick and only discover the problem during infertility investigations.
Tubal disease often hides in plain sight—most women with blocked tubes never had any clear warning signs.
Tuberculosis deserves special mention. In India, pelvic tuberculosis remains a significant cause of tubal infertility. It travels through the bloodstream and can cause permanent, sometimes invisible, damage to the fallopian tubes.
How Can You Find Out if Your Tubes Are Blocked?
For many couples, the hardest part is not knowing. Thankfully, today there are several reliable ways to check whether your fallopian tubes are open and functioning:
1. Hysterosalpingogram (HSG)
This is the most common test for checking tubal patency (openness). An HSG is a special X-ray taken after injecting a dye into the uterus. The dye outlines the shape of the womb and tubes, letting the doctor see if the tubes are open or blocked. It is done just after your period ends, typically on day 6 or 7, when the uterine lining is thin.
You may be given a mild painkiller and antibiotic before the procedure. A thin tube or balloon catheter is gently inserted into the cervix, and the dye is injected. The movement of the dye is tracked by X-ray images. If the dye flows freely from the uterus, through the tubes, and spills into the abdomen, this is a good sign—the tubes are open.
At least three images are usually taken: one to show the uterine cavity, one as the dye enters the tubes, and a delayed image to check if the dye has spilled out into the abdominal cavity.
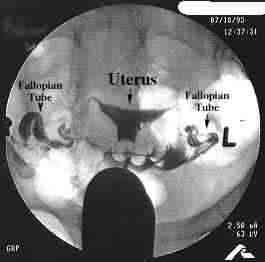 Fig 2. Normal HSG findings (the dye appears black and outlines a normal cavity and fallopian tubes)
Fig 2. Normal HSG findings (the dye appears black and outlines a normal cavity and fallopian tubes)
If the tubes are blocked at the beginning (cornual block), the dye does not enter them at all. If the block is at the end (fimbrial block), the tube fills up, but the dye cannot escape into the abdomen. Sometimes, a swollen tube (hydrosalpinx) is seen, which is a sign of fluid buildup due to blockage.
2. Blood Tests for Chlamydia Antibodies
Because chlamydia is a common cause of tubal damage, some doctors may order a blood test to check for past infection. A positive result means there is a higher risk of tubal disease, but it is not a definitive diagnosis.
3. Laparoscopy
This is the “gold standard” for diagnosing tubal problems. During a laparoscopy, a thin telescope (laparoscope) is inserted through a small cut in the belly button, letting the doctor look directly at the tubes, ovaries, and pelvis. Dye may be injected to watch its movement through the tubes. Laparoscopy can also spot adhesions or other hidden problems that an HSG cannot show.
Sometimes, a laparoscopy is recommended only if the HSG is abnormal or if there are other signs of pelvic disease. While it is more invasive than the other tests, it gives the most complete picture.
What Are the Limitations of Tubal Testing?
No test is perfect, and this is especially true with tubal assessment. Both HSG and laparoscopy can show you whether your tubes are open or blocked, but they cannot always tell you if an “open” tube is actually healthy or working well. The HSG, for example, might show dye spilling out, but if the tube is damaged on the inside (for example, if the cilia are destroyed), natural conception might still be impossible.
 Fig 3. Laparoscopy shows a large hydrosalpinx on the right side
Fig 3. Laparoscopy shows a large hydrosalpinx on the right side
HSG can sometimes give false alarms. For example, a muscle spasm in the uterus can make it look like the tube is blocked when it is actually open. Or, in rare cases, the dye can leak through a tear, making a blocked tube appear open. Laparoscopy too has its limitations: it may not always reveal why the blockage happened, except in cases where visible signs like tubercles from tuberculosis are present.
Just because your tubes are open on a test does not always mean they work as they should.
This is why getting expert, honest advice is so valuable. At Malpani Infertility Clinic, we believe in giving our patients the whole picture—so you can make informed decisions and not waste precious time or emotional energy.
Recent Advances: What Else Can Be Done for Tubal Factor?
While the basics of tubal testing have not changed in decades, some exciting innovations have made both diagnosis and treatment more precise. These include:
- Fluoroscopic-Guided Tubal Cannulation: Using a special X-ray machine (image intensifier), doctors can guide a thin catheter into the tubes to clear minor blockages caused by mucus plugs, sometimes restoring tubal patency immediately.
- Sonosalpingography: This is a gentle, ultrasound-based test where a small amount of fluid is injected through the cervix, and its movement through the tubes is seen on an ultrasound screen. It is less invasive and can be done in the clinic, offering quick reassurance when normal.
- Tuboscopy: During laparoscopy, a tiny telescope can be inserted directly into the fimbrial end of the fallopian tube to inspect its lining. This gives direct information about the tube’s health, something traditional tests cannot do.
- Falloposcopy: A very fine, flexible scope is threaded through the uterus and into each fallopian tube. This lets the doctor see the entire length of the tube from inside, helping assess the extent of damage and whether repair is possible. It is a sophisticated technique, available only at select centers.
These advanced tools are not needed for everyone, but they can be life-changing for couples with stubborn or unexplained tubal problems. If you are unsure whether you need advanced testing, a focused consultation with an expert can help you weigh the options.
Frequently Asked Questions
Q: What symptoms suggest my fallopian tubes might be blocked?
A: Most women with tubal blockage have no symptoms at all. The most common sign is difficulty getting pregnant despite regular cycles and ovulation. Rarely, a past history of pelvic infections or abdominal surgery may be a clue.
Q: Is an HSG painful or dangerous?
A: An HSG can cause cramping and discomfort when the dye is injected, but taking a painkiller beforehand helps most women. The risk of infection is low, especially if antibiotics are used. Talk to your doctor if you have concerns about pain or risk.
Q: If my tubes are blocked, can they be repaired?
A: In some cases, minor blockages (especially at the beginning of the tube) can be opened with special catheters. However, severe damage or scarring is often permanent. In such cases, IVF offers the best chance for pregnancy.
Q: Does having open tubes guarantee I will get pregnant?
A: Unfortunately, no. Tubes may be open but still not function properly (for example, if the cilia are damaged). This is why sometimes IVF is recommended even when tests show “open” tubes.
Q: Should I do all the tests at once?
A: Not always. Most couples start with an HSG. Further tests like laparoscopy or advanced imaging are only needed if there is a clear problem or if you have risk factors for tubal disease.