Is Endometriosis Stealing Your Dreams of Motherhood?

- Endometriosis is a chronic condition where tissue similar to the uterine lining grows outside the uterus, causing pain and inflammation.
- Symptoms vary widely and can include severe period pain, pain during sex, fatigue, digestive issues, and sometimes infertility.
- About one third of women with endometriosis struggle with getting pregnant.
- The severity of pain or symptoms does not always match what doctors see on scans or during surgery.
- Endometriosis can affect anyone, regardless of lifestyle, and is not just a 'bad period.'
You are not imagining it. The confusion, the frustration, the loneliness, it is all real. Maybe you have spent years dreading your periods, doubled over in pain, baffled by why your cramps are so much worse than everyone else’s. Or maybe you are exhausted by the endless rounds of “when are you having a baby?” from well-meaning relatives, not knowing how to explain that your body just will not cooperate. If endometriosis is stealing your peace or your hope for motherhood, you are not alone, and you deserve honest answers and a path forward.
What Really Is Endometriosis?
Endometriosis is not just a “bad period.” It is a chronic condition where tissue similar to the lining inside your uterus (the endometrium) starts growing outside it, on your ovaries, fallopian tubes, bowels, or anywhere in your pelvic cavity. Every month, these patches react to your hormones, swell, and bleed, just like your uterine lining. But unlike a normal period, this blood has nowhere to go. The result: pain, inflammation, and, over time, the formation of sticky bands called adhesions that can tangle up your pelvic organs.
Many women develop endometriosis in their twenties and thirties, especially if they have delayed pregnancy. It is sometimes unfairly dubbed a “career woman’s disease,” but the truth is it can affect anyone, regardless of lifestyle. What makes it even harder is that it can sneak up quietly, causing barely any symptoms in some women, while for others, it is an all-consuming, life-altering battle.
Why does it happen? No one can say for sure. Some experts think it might be due to “retrograde menstruation,” where menstrual blood flows backwards through the fallopian tubes into the pelvis. Others suspect genetics, immune problems, or even environmental factors. It is an enigma that medical science is still trying to unravel.
Recognizing the Symptoms: It Is Not “Just in Your Head”
One of the most frustrating things about endometriosis is that it does not look the same in every woman. You might have severe pain, or none at all. The degree of suffering does not always match what a doctor sees on a scan or during surgery.
- Severe period pain (dysmenorrhea): Pain that starts before your period and gets worse as the years go by.
- Pain during sex (dyspareunia): Sharp or deep pain, not just discomfort.
- Unexplained fatigue: Feeling drained, even when you have slept well.
- Bloating or digestive issues: Some women experience bowel pain, constipation, or diarrhea, especially during their cycle.
- Infertility: For about a third of women with endometriosis, getting pregnant is a real struggle.
- Painful urination or bowel movements: Particularly during your period.
Some women have “chocolate cysts” (endometriomas) on their ovaries, filled with old blood. Others develop adhesions that glue their organs together, making periods and intercourse excruciating. But even if your pelvic scans look normal, your pain is still real.
The pain of endometriosis is not just physical, it can leave you feeling isolated, misunderstood, and exhausted.
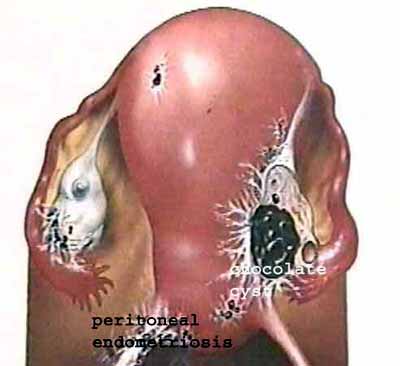 Fig 1. Schematic, showing a chocolate cyst (endometrioma) in the right ovary; and peritubal adhesions because of endometriosis
Fig 1. Schematic, showing a chocolate cyst (endometrioma) in the right ovary; and peritubal adhesions because of endometriosis
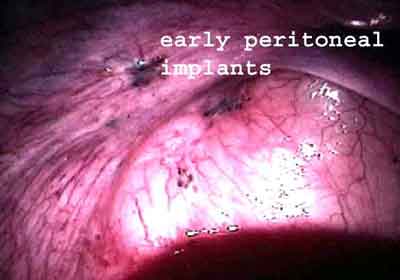 Fig 2. Laparoscopy, showing minimal endometriosis, in the form of powder-burn deposits.
Fig 2. Laparoscopy, showing minimal endometriosis, in the form of powder-burn deposits.
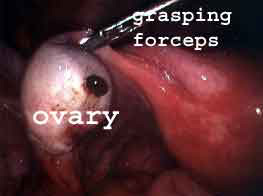 Fig 3. Laparoscopy, showing a small chocolate cyst in the left ovary. This can be very easy to miss, so a careful multiple puncture laparoscopy is essential to make an accurate diagnosis of endometriosis.
Fig 3. Laparoscopy, showing a small chocolate cyst in the left ovary. This can be very easy to miss, so a careful multiple puncture laparoscopy is essential to make an accurate diagnosis of endometriosis.
How Does Endometriosis Affect Fertility?
If you are struggling to conceive, endometriosis might be part of the reason. But understanding how is not always straightforward. Sometimes, the inflammation caused by endometriosis releases chemicals (like cytokines) that can interfere with the growth and release of healthy eggs, the movement of sperm, or even implantation of an embryo. In more severe cases, the adhesions (scar tissue) can tie up your ovaries and tubes, making it physically hard for eggs to travel or be picked up during ovulation. Chocolate cysts can also sap the health of your ovaries, damaging egg quality and supply.
But here is the twist: some women with severe endometriosis get pregnant easily, while others with only mild disease struggle for years. And sometimes, endometriosis is just a bystander, the real fertility problem could be elsewhere, like poor sperm quality or ovulation issues. That is why a careful, honest evaluation is so important.
women with endometriosis may face infertility, but many still conceive naturally or with help.
Diagnosis: Why Is It So Difficult?
If you have ever felt dismissed by a doctor who said “it is just bad periods” or “maybe it is stress,” you are not alone. Endometriosis can be hard to spot. Ultrasound scans may show large chocolate cysts, but smaller patches or subtle adhesions are often invisible on imaging. For years, the only way to confirm endometriosis was through a surgical procedure called laparoscopy, where a tiny camera is inserted to look for the telltale lesions.
Today, better ultrasound techniques can help identify suspicious cysts or pelvic changes, but they are not foolproof. If you have persistent symptoms and no clear diagnosis, do not be afraid to push for answers. Your pain is valid.
Getting a diagnosis can be both a relief and a shock, but it is the first step toward taking back control.
Doctors often use the ASRM system to stage endometriosis from I (minimal) to IV (severe). This helps plan treatment, but remember: the stage does not always match the pain or the impact on fertility.
Treatment Options: What Actually Works (and What Does Not)?
This is where a lot of women get lost in the medical maze, sometimes undergoing unnecessary treatments that waste time or even lower their chances of pregnancy. Here is the no-nonsense truth:
- Hormonal medicines (like birth control pills or GnRH analogues): These can help control pain by suppressing your periods, but they do not improve fertility. In fact, you cannot conceive while taking them. That is why, if your main goal is to have a baby, medicines alone are not the answer.
- Surgery (laparoscopy): This can remove endometriosis patches, release adhesions, and drain chocolate cysts. In some women, especially those with severe pain or large cysts, it brings real relief. But surgery is not always helpful for fertility, and sometimes it can even damage healthy ovarian tissue, reducing your egg supply. Too much surgery can do more harm than good.
- Superovulation with Intrauterine Insemination (IUI): If your tubes are open and your ovarian reserve is good, this is often the next step if you do not conceive naturally.
- In Vitro Fertilization (IVF): IVF bypasses many of the problems caused by endometriosis, especially if your tubes are blocked, your ovarian reserve is low, or you have failed other treatments. It is not a cure for endometriosis, but it can be a highly effective way to achieve pregnancy.
If you are being advised surgery, always check your AMH level (a simple blood test that tells you about your egg supply). If your ovarian reserve is already low, especially if you are older, have had previous surgeries, or have big cysts, think twice before another operation. Sometimes, draining a cyst under ultrasound guidance is safer for your ovaries than cutting it out.
What nobody tells you: treatment has to be tailored to you, your age, your symptoms, your fertility goals, and your ovarian reserve. There is no “one size fits all.”
Living with Endometriosis: You Are Not Alone
Endometriosis is not just a physical condition, it affects your mind, your relationships, and your sense of self. The shame of not being able to explain your pain, the guilt of letting people down, the fear that you will never become a mother: these are burdens you should never have to carry in silence.
Many women find strength in connecting with others who “get it.” At Malpani Infertility Clinic, we have seen countless women who were told their pain was imaginary, their infertility hopeless. With honest guidance, advanced diagnostics, and individualized care, many of them have gone on to build the families they dreamed of. We believe in empowering you with knowledge, not just about the disease, but about your real options.
If you are struggling to make sense of your symptoms, frustrated by failed treatments, or just want a second opinion on your options, you are always welcome to speak to an expert fertility advisor at Malpani Infertility Clinic.
Frequently Asked Questions
Q: Can I get pregnant naturally if I have endometriosis?
A: Many women with endometriosis do conceive naturally, especially if the disease is mild and their tubes are open. However, about one in three may struggle and need fertility support. Early evaluation helps you make the best choices.
Q: Does endometriosis always cause pain?
A: No. Some women have severe endometriosis with little or no pain, while others with only mild disease suffer intensely. Pain is not always a reliable guide to how much disease is present.
Q: Will hormonal medicines help me get pregnant?
A: No. Hormonal treatments can suppress symptoms but do not boost fertility. In fact, you cannot get pregnant while on these medications. If fertility is your goal, other options are better suited.
Q: Is surgery for endometriosis always necessary?
A: Not always. Surgery can relieve pain or remove large cysts, but it is not always needed for fertility. In some cases, surgery can lower your ovarian reserve. Always check your AMH level and discuss all options before proceeding.
Q: What tests help diagnose endometriosis?
A: Diagnosis can start with your symptoms and a pelvic exam. Ultrasound can reveal chocolate cysts, but laparoscopy is often needed to see small or hidden lesions. A careful, experienced approach is key for accurate diagnosis.
Q: Can IVF help if I have endometriosis?
A: Yes. IVF is a proven option for women with endometriosis, especially if other treatments have failed or if there is significant pelvic damage. It bypasses many obstacles caused by endometriosis and can lead to successful pregnancy.
Q: Should I be worried about passing endometriosis to my daughter?
A: There is some genetic risk, but not every daughter of a woman with endometriosis will develop the disease. Early awareness and support can make a big difference if symptoms arise.