What Every IVF Patient Should Know About Embryo Grading

When you finally reach the IVF stage, you’re already carrying the invisible weight of years of hope, disappointment, and endless questions. You’ve learned the language of scans and medications, but the moment you hear “embryo grading,” it feels like you’re back in the dark. If you’ve ever wondered what really happens inside the IVF lab, or felt your heart race when your doctor started discussing “Grade A” or “fragmentation” as if these words decide your entire future, you are not alone. At Malpani Infertility Clinic, we believe you deserve real answers—no sugar-coating, no jargon, just the truth that helps you make better decisions for your own journey.
What Does Embryo Grading Really Mean for You?
Most couples starting IVF have endless questions about scans, medications, and hormones, but what happens to your eggs and sperm after retrieval often feels like a mystery. Embryo grading is the process we use to assess which embryos are most likely to result in a healthy pregnancy. It’s not just a technical step: it’s the moment where science, chance, and your deepest hopes meet.
At Malpani Infertility Clinic, we show every patient their own embryos before transfer, so you can see for yourself what’s happening and feel more in control. Here’s how we break down embryo grading, so you can finally understand—and not just worry about—what’s happening in the lab.
How Do We Grade Embryos? Breaking Down the Process
Embryo grading changes as the embryo develops, and at Malpani Infertility Clinic, we use transparent grading systems for both Day 3 and Day 5 embryos. Here’s what you need to know:
- Day 2 and Day 3 (Cleavage Stage): We look at how many cells the embryo has, how regularly those cells are sized, and whether there’s any “fragmentation”—tiny bits of cell debris that can signal problems.
- Day 5 and Day 6 (Blastocyst Stage): The embryo becomes a blastocyst, with distinct cell layers and a fluid-filled cavity. Here, we assess the size and expansion of the cavity, the quality of the inner cell mass (which forms the baby), and the quality of the trophectoderm (which forms the placenta).
Understanding Day 2 and Day 3 Embryo Grading
On Day 2, embryos should ideally have 2-4 cells, and by Day 3, 6-10 cells. These cells are called blastomeres. The more regular and symmetrical the cells, and the less fragmentation present, the higher the grade. Here’s how we break it down:
- Grade A: Even-sized cells, less than 10% fragmentation. This is the gold standard.
- Grade B: Even-sized or nearly even cells, but more than 10% fragmentation.
- Grade C: Uneven cell size and more than 10% fragmentation.
- Grade D: Irregular blastomeres, more than 20% fragmentation.
Even an embryo with some fragments can become a healthy baby; grading is about odds, not guarantees.


2-Cell (Day 2 embryo) 4-Cell (Day 2 embryo)

 6-Cell (Day 3 Embryo) 10-Cell (Day 3 Embryo)
6-Cell (Day 3 Embryo) 10-Cell (Day 3 Embryo)
We also consider cell regularity. Ideally, all blastomeres should be the same size. If not, the closer they are in size, the better.

4-Cell Embryo with blastomeres of unequal sizes. This is a Grade B embryo.
Fragmentation is another concern: this is when small pieces break off from the main cells, usually as a result of natural cell death. Less is better, but some fragmentation is very common.

10-Cell Grade A embryo: Regular blastomeres, no fragmentation.
 10-Cell Grade B embryo: Regular blastomeres, > 10% fragmentation.
10-Cell Grade B embryo: Regular blastomeres, > 10% fragmentation.
 8-Cell Grade C embryo: Irregular blastomeres, > 10% fragmentation.
8-Cell Grade C embryo: Irregular blastomeres, > 10% fragmentation.
 8-Cell Grade D embryo: Irregular blastomeres, > 20% fragmentation.
8-Cell Grade D embryo: Irregular blastomeres, > 20% fragmentation.
Many couples panic if their embryos aren’t “Grade A.” The truth is, many beautiful babies are born from embryos that looked “average” or even “poor” in the lab. Grading tells us about chances, not outcomes.
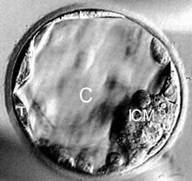
Blastocyst (Day 5/6) Grading: Looking Deeper
By Day 5, the embryo has become a blastocyst. Here’s how we grade these more complex embryos:
- Cavity Expansion (1-6): How much the cavity has expanded and whether the embryo is hatching from its shell (zona pellucida).
- Inner Cell Mass (A, B, C): The cluster of cells that becomes your baby. “A” is tightly packed and clearly defined.
- Trophectoderm (A, B, C): The outer layer that becomes the placenta. “A” is a uniform, cohesive layer of many cells.

The inner cell mass is marked as ICM, the cavity as C, and the trophectoderm as T. Early blastocysts are just beginning to form these structures.


- Early Blastocysts: Cavity fills less than half the embryo’s volume (Grade 1AA, 1AB, 1BA...)
- Intermediate Blastocysts: Cavity fills more than half the embryo’s volume (Grade 2AA, 2AB, 3AA...)
- Expanded Blastocysts: Cavity completely fills the embryo’s volume (Grade 4AA, 4AB...)
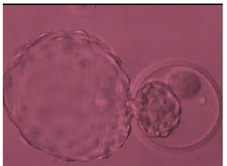
- Hatching Blastocysts: Embryo is breaking out of its shell (Grade 5AA, 5AB...)
- Completely Hatched Blastocysts: Embryo is fully out of the shell (Grade 6AA, 6AB...)




Success rate per transfer for top-quality 5AA or 6AA blastocysts, but even lower grades can succeed.
Common Questions IVF Patients Ask About Embryo Grading
When you’re waiting for updates from the lab, every detail feels life-or-death. Here are the answers to the questions you’re probably too anxious to ask—or have been given incomplete answers about elsewhere.
-
How many embryos do you transfer?
At Malpani Infertility Clinic, we usually recommend transferring a single top-quality blastocyst on Day 5. This minimizes the risk of multiple pregnancies, which can be risky for both mother and babies. We individualize for your age, embryo quality, and unique situation.
-
Why is my embryo quality not "perfect"?
Embryo quality depends on the egg, the sperm, and the lab conditions. In India, many poor results are simply due to substandard labs—especially if the clinic won’t show you embryo photos. A good clinic is transparent. If you see poor fertilization after IVF, sperm may be the issue. If it's after ICSI, eggs are usually to blame. Poor sperm do not affect embryo quality if ICSI is done.
-
Why do some embryos grow slowly?
Not all embryos develop at the same pace, even from the same couple. Slow growth does reduce the chances, but slow-growing embryos have still resulted in healthy babies. Don’t lose hope just because your embryos aren’t “textbook.”
-
Why is my fertilization rate low?
- Poor fertilization after IVF usually means sperm issues. We recommend ICSI next time.
- Poor fertilization after ICSI usually points to egg quality.
- Very rarely, a total failed fertilization after ICSI can mean a rare sperm disorder (globozoospermia), needing specialized techniques.
-
If embryo quality is “bad,” what are the chances of pregnancy?
Even lower-grade embryos sometimes implant and result in healthy babies. The odds are reduced, but not zero. No one can give you a precise prediction—only honest probabilities.
-
Why not transfer more than one embryo?
Many believe “more is better,” but transferring more than one doesn’t improve your individual success rate—it just increases the risk of twins or triplets, which carry much higher risks. If you have good embryos, it’s safer to transfer one and freeze the rest.
-
Does transferring a Day 5/6 blastocyst increase success?
Yes. Blastocyst transfers allow us to select embryos with the highest developmental potential. Extended culture lets the embryos “compete,” so only the best make it to Day 5, and we can freeze the rest for future use.
-
What about sequential embryo transfer?
Transferring embryos on both Day 3 and Day 5 in the same cycle doesn’t improve pregnancy chances and wastes embryos. Good clinics avoid this practice.
-
How do you prevent embryos from being mixed up?
Every single dish, tube, and incubator at our clinic is labeled with the patient’s name, and every step is double-checked by both the embryologist and nurse. Your embryos are never out of sight or unaccounted for.
-
How long can embryos be safely frozen?
There’s no strict time limit. As long as storage conditions are maintained (which we monitor constantly), embryos can be frozen for years. There is an annual storage fee, but no “expiry date.”
-
Why do some embryos have an odd cell number like 3?
Cell division is continuous. If we check at a moment between divisions, you might see an odd number like 3 or 5. This is normal and not a cause for concern.
-
Why don’t all normal-looking embryos implant?
Looks can be deceiving. Even if an embryo appears perfect, up to 60% of all human embryos (even in young couples) are genetically abnormal. This is simply a part of nature’s inefficiency.
-
Do we need to test embryos genetically before transfer?
Routine genetic testing (PGD/PGS or PGD) is only advised if there’s a known genetic risk. It’s not a magic solution and isn’t required for most couples.
-
What happens to embryos that don’t implant?
They stop growing and are reabsorbed by the body. There’s no pain, no bleeding, and it doesn’t affect your future chances.
What Nobody Tells You About Embryo Grading
It’s easy to get lost in the alphabet soup of grades and percentages, but here’s what really matters:
- Grading is just a tool. It helps us pick the embryos with the best odds, but it’s not a prophecy.
- Even lower-grade embryos have made parents out of people who almost gave up hope.
- If your clinic isn’t showing you your embryo photos or explaining their grades, ask why. You have a right to full transparency.
- Every step of IVF is about increasing your odds, not guaranteeing a result. No clinic—no matter how famous—can promise a baby. Anyone who does is not being honest.
Frequently Asked Questions
Q: What is embryo grading, and why does it matter?
A: Embryo grading is how embryologists assess embryos’ potential to implant and become a baby. It helps doctors decide which embryo is best for transfer, but it’s not a guarantee of success.
Q: Can a lower-grade embryo become a healthy baby?
A: Yes. Many healthy babies have been born from embryos that looked “average” or “poor” in the lab. Grading is about probabilities, not certainties.
Q: Why is single embryo transfer usually recommended?
A: Single embryo transfer lowers the risk of twins or higher-order multiples, which can be dangerous for both mother and babies. The best embryo is chosen to maximize your chance of a healthy singleton pregnancy.
Q: How are embryos labeled to prevent mix-ups?
A: Every container, dish, and incubator is clearly labeled with the patient’s name, and all steps are double-checked. Strict protocols mean your embryos are always safe and accounted for.
Q: How long can embryos stay frozen?
A: Embryos can be frozen for years with no loss of quality, as long as storage is maintained. There’s no official time limit.
Q: Does embryo grading guarantee pregnancy?
A: No. Higher grades mean higher chances, but success depends on many factors, including uterine receptivity and genetics.
Q: Should I ask my clinic to show me my embryo photos?
A: Absolutely. Transparency is a sign of a high-quality, ethical clinic. You have a right to see and understand your embryos.
Q: Is genetic testing of embryos always necessary?
A: No. Genetic testing is only advised if you have a known genetic risk or history of repeated IVF failures or miscarriages. Most couples do not need it.